Postpartum haemorrhage: various method of management in arural tertiary care hospital
Abstract
Introduction: Post-partum haemorrhage is defined as blood loss from the genital tract, exceeding 500ml within 24hours of vaginal delivery and 1000ml during caesarean section. It is also now a day defined as any blood loss that has a potential to produce or produces hemodynamic instability. Massive obstetric haemorrhage is a major cause of maternal mortality and morbidity worldwide.
Aims and Objectives: Objective of the study is to evaluate the most common etiology and method of management of Postpartum Haemorrhage in a rural tertiary care hospital of SAH &RC.
Materials and Methods: A prospective study was done from June 2017 to June 2018 in Department of Obstetrics and Gynaecology at Adichunchanagiri Institute of Medical sciences, Bellur, Karnataka, India. The study included all cases of normal vaginal deliveries, assisted vaginal deliveries and Caesarean section.
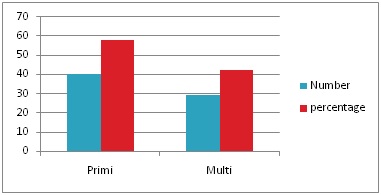
Result: A total of 1877women were delivered. Out of which 923 (49.17%) women delivered vaginally and 954 (50.82%) women delivered through cesarean section. Out of 1877 delivered women, 69 (3.67%) developed PPH. out of 69(3.79%), 66(95.65%) had atonic PPH and 3(4.34%) had traumatic PPH. out of 66 atonic PPH cases 54(81.81%) managed medically. Other modalities were B lynch suture 7(10.6%), Hayman suture 2(3.03%), suction cannula 1(1.51%), internal iliac artery ligation 1(1.51%), peripartum hysterectomy 1(1.51%). Most of the cases have been managed medically.
Conclusion: In an era with availability of excellent uterotonics and active management of third stage of labor even today PPH stands first as the cause of maternal mortality and morbidity.This study highlights the existing variable practices for management of PPH. Haemorrhage associated mortality can be prevented by critical judgment and early intervention.
Downloads
References
2. WHO. A newsletter of world wide activity. Making Pregnancy Safer. 2007;4:1-8.
3. Muhammad S, Chandraharan E. Chapter 23 postpartum haemorrhage, Aria’s practical guide to high risk pregnancy and delivery, a south Asian perspective, Elsevier publication, 4th ed;389-98.
4. Shaikh S, Bano N, Talpur S, Balouch R. Postpartum Hemorrhage: An Experience at Tertiary Care Hospital, Hyderabad. MC. 2013;19(1):44-7.
5. Sheikh L, Najmi N, Khalid U, Saleem T. Evaluation of compliance and outcomes of a management protocol for massive postpartum hemorrhage at a tertiary care hospital in Pakistan. BMC Pregnancy Childbirth. 2011;11(1):28,1-7.
6. André Lalonde FIGO Safe Motherhood and Newborn Health (SMNH) Committee. Prevention and treatment of postpartum hemorrhage in low‐resource settings. International Journal of Gynecology and Obstetrics 117 (2012) 108–118 doi:10.1016/j.ijgo.2012.03.001
7. World Health Organization. The Prevention and Management of Postpartum Haemorrhage. Report of a Technical Working Group, Geneva, 3-6 July, 1989. Unpublished document. WHO/ MCH/90.7. Geneva: World Health Organization, 1990
8. Rath W, Hackethal A, Bohlmann MK. Second-line treatment of postpartum haemorrhage (PPH). Arch Gynecol Obstet. 2012 Sep;286(3):549-61. doi: 10.1007/s00404-012-2329-z. Epub 2012 May 4.[pubmed]
9. Mousa HA, Blum J, Abou El Senoun G, et al. Treatment for primary postpartum haemorrhage. Cochrane Database Syst Rev. 2014 Feb 13;(2):CD003249. doi: 10.1002/14651858.CD003249.pub3.[pubmed]
10. Sheikh L, Najmi N, Khalid U, et al. Evaluation of compliance and outcomes of a management protocol for massive postpartum hemorrhage at a tertiary care hospital in Pakistan. BMC Pregnancy Childbirth. 2011 Apr 13;11:28. doi: 10.1186/1471-2393-11-28.
11. Krishna H, Chava M, Jasmine N, Shetty N: Patients with postpartum hemorrhage admitted in intensive care unit: Patient condition interventions, and outcome. J Anaesthesiol Clin Pharmacol 2011, 27(2):192-4.doi10.4103/0970-9185.81826.
12. Condous GS, Arulkumaran S. Medical and conservative surgical management of postpartum hemorrhage. J ObstetGynaecol Can. 2003 Nov;25(11):931-6.[pubmed]
13. Csorba R. Management of post partumhaemorrhage. Orv Hetil. 2012 Apr 29;153(17):643-8. doi: 10.1556/OH.2012.29330.[pubmed]
14. Rath W, Hackethal A, Bohlmann MK. Second-line treatment of postpartum haemorrhage (PPH). Arch Gynecol Obstet. 2012 Sep;286(3):549-61. doi: 10.1007/s00404-012-2329-z. Epub 2012 May 4.[pubmed]
15. Management of postpartum hemorrhage. http://www.drplace.com/ Management_of_postpartum_hemorrhage.16.22850.htm.
16. Prendiville W, Elbourne D, McDonald S. Active versus expectant management in the third stage of labour. Cochrane Database Syst Rev 2009(3):CD000007. doi:10.1002/14651858.CD000007.pub2.
17. Prendiville WJ, Harding JE, Elbourne DR, Stirrat GM. The Bristol third stage trial: active versus physiological management of third stage of labour. BMJ 1988;297(6659):1295–300. PMID:3144366
18. Rogers J, Wood J, McCandlish R, et al. Active versus expectant management of third stage of labour: the Hinchingbrooke randomised controlled trial. Lancet. 1998 Mar 7;351(9104):693-9. DOI:10.1016/S0140-6736(97)09409-9.[pubmed]
19. United Nations. United Nations Millennium Development Goals 2000. http://www.un.org/millenniumgoals. Accessed September 15, 2011.
20. Tasneem F, Sirsam S, Shanbhag V. Clinical study of post partumhaemorrhage from a teaching hospital in Maharashtra, India. Int J Reprod Contracept ObstetGynecol2017 Jun;6(6):2366-2369.
21. Pranita Solanke, Swapnali Patil, Prithviraj Patil. Study of Postpartum haemorrhage in tertiary care centre. International Journal of Scientific and Research Publications, Volume 4, Issue 10, October 2014 1 ISSN 2250-3153 www.ijsrp.org
22. Calvert C, Thomas SL, Ronsmans C, et al. Identifying regional variation in the prevalence of postpartum haemorrhage: a systematic review and meta-analysis. PLoS One. 2012;7(7):e41114. doi: 10.1371/journal.pone.0041114. Epub 2012 Jul 23.[pubmed]
23. Sabrina D, Craigo, Peter S, Kapernick. Postpartum hemorrhage and abnormal puerperium. Current Obstetrics and Gynecology logic diagram.6th ed. London: Appleton and Lange; 1987.p 574–82.
24. Japaraj RP, Raman S. Sengstaken-Blakemore tube to control massive postpartum haemorrhage. Med J Malaysia. 2003 Oct;58(4):604-7.
Copyright (c) 2019 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative





