Comparative study of different routes of hysterectomy
Abstract
Background: To compare the various routes of hysterectomy and find the most commonly performed hysterectomy type and the various complications associated with each.
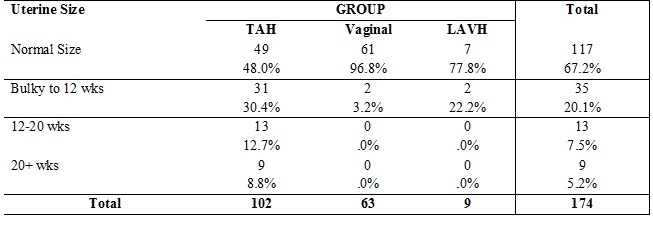
Methods: This prospective study was carried out in the department of Obstetrics and Gynaecology, N.S.C.B. medical College, Jabalpur during June 2007 to August 2008. A total of 174 cases included in the study. The women were divided into three groups depending on the surgical approach: the abdominal group consisted of women who underwent hysterectomy via a suprapubic or median incision; the laparoscopically assisted vaginal hysterectomy (LAVH) group consisted of women who underwent vaginal hysterectomy assisted by laparoscopic procedure (excluding uterine artery ligation) and vaginal hysterectomy.
Results: The indications of hysterectomy differed among groups. Four main indications in the cases coming to medical college: Fibroid, DUB, Genital prolapse and PID. Prolapse was a more frequent indication for vaginal hysterectomies; however, abdominal hysterectomies or Laparoscopically assisted vaginal hysterectomies were used in 16 out of the 76 cases that involved only prolapse. Fibroids were more frequently an indication for abdominal or laparoscopic assisted vaginal hysterectomy.
Conclusion: The vaginal route has significant advantages over LAVH and abdominal hysterectomy and should be the route of first choice. Hence there is a tremendous scope for improvement by careful preoperative assessment, meticulous surgical techniques and proper postoperative care in order to reduce the complication rate.
Downloads
References
2. Thomas G. Stovall, Vaginal, Abdominal, Laparos copic- Assisted Hysterectomy Book of Gynecologic Surgery 403-407.
3. Thomas W. Mc Donald, Hysterectomy. Indications, types and alternatives, Book of Gynecology, 1024-1029.
4. Reich H, De caprio J, Mc Glynn F. Laparoscopic Hysterectomy. Gynecology Surgery1989; 213-226.
5. David-Montefiore E, Rouzier R, Chapron C, et al. Surgical routes and complications of hysterectomy for benign disorders: a prospective observational study in French university hospitals. Hum Reprod. 2007 Jan; 22(1):260-5. Epub 2006 Sep 1. DOI:10.1093/humrep/del336.[pubmed]
6. Kovac SR. Hysterectomy outcomes in patients with similar indications. Obstet Gynecol. 2000 Jun;95(6 Pt 1):787-93.[pubmed]
7. Van Den Eden, Stephen K, Glasser Mark: Quality of life, health care utilization and costs among women undergoing hysterectomy in a manged care setting. American Journal of Obstetrics and Gynecology. 91-100, Jan 1998.
8. Kang YP, Lee SN , Kang CG : Laparoscopically assisted vaginal hysterectomy : A review of 43 cases. Korean J. Obstetrics and Gynecology, 1998 : 2621-2624.[pubmed]
9. Michel Cosson, Malik Boukerrou, Eric Lambaudic : Hysterectomy for benign lesions : What is left for the abdominal route. Journal of Gynecology Surgery, Dec. 2001: 109-114.
10. Ronald M,: What I have learned from performing vaginal hysterectomy. Medscape, Obstetrics and Gyneco. & Women’s health, 2003.[pubmed]
11. Malinowski A, Bobin L, Ma Clolak – Blewniewska G : Significance of laparoscopic assistance in vaginal hysterectomy. Jr. Article, Ginekol Pol 2005, 20-7.
12. Boukerrou M, Lambaudie E, Collinet P, et al. A history of cesareans is a risk factor in vaginal hysterectomies. Acta Obstet Gynecol Scand. 2003 Dec;82(12):1135-9.[pubmed]
13. Councell RB, Thorp JM Jr, Sandridge DA, et al. Assessments of laparoscopic-assisted vaginal hysterectomy. J Am Assoc Gynecol Laparosc. 1994 Nov; 2(1):49-56.[pubmed]
14. Bronitsky C, Stuckey SJ. Complications of laparoscopic-assisted vaginal hysterectomy. J Am Assoc Gynecol Laparosc. 1995 May;2(3):345-7.[pubmed]
15. Obstetrics – Gynecology News, by Nacy Wals: Hysterectomy Guidelines often are not followed. 2000.[pubmed]
16. Edozien LC. Hysterectomy for benign conditions. BMJ. 2005 Jun 25;330(7506):1457-8. DOI:10.1136/bmj.330.7506.1457.[pubmed]
17. Mukherjee SN. Role of hysterectomy and its alternatives in benign uterine diseases. J Indian Med Assoc. 2008 Apr; 106(4):232-4, 236.[pubmed]
18. Kovac SR, Barhan S, Lister M, et al. Guidelines for the selection of the route of hysterectomy: application in a resident clinic population. Am J Obstet Gynecol. 2002 Dec; 187(6):1521-7.[pubmed]
19. Bobin L, Maciołek-Blewniewska G, Malinowski A. [Operating time of laparoscopically assisted vaginal hysterectomy (LAVH)--the causative factors and the course of the postoperative period]. Ginekol Pol. 2007 Mar; 78(3):204-9.
Copyright (c) 2018 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative





