A retrospective study of urinary tract infections in post-operative gynae-oncology patients in a tertiary care hospital of Chhattisgarh
Abstract
Introduction: Urinary tract infections (UTIs) are second most common hospital acquired infections. There are multiple risk factors for UTIs. Patients with gynecological malignancies undergoing treatment are more predisposed for getting UTIs as they have multiple risk factors including prolong duration of urinary catheterization.
Objective: This retrospective study was done to find the incidence and risk factors related to the occurrence of urinary tract infections (UTIs) inpost-surgerygynecological cancer patients.
Methods: Data of Ninety two women was collected and reviewed with domains covering known risk factors for the occurrence of urinary tract infections. Bacteriuria was defined as > 105 colony-forming units per milliliter.
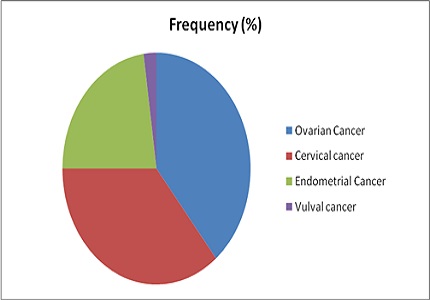
Results: 38% of women had UTI post-operatively. Among them, 71.4% infections were Escherichia coli. Catheter in situ for 7 days duration was found to be highly significant in the occurrence of UTI (p<0.01; OR 2.62). A positive correlation was found between the duration of the catheter in situ and type of UTI (P < 0.01).
Conclusions: Urinary catheterization is known to be related to hospital-acquired infection, and risk can be reduced by a shorter duration of catheterization post surgery. Gynecologists need to be more aware of this risk and identify women who are more likely to be catheterized for longer and use preventive strategies for managing infection, such as silver nitrite-lined catheters.
Downloads
References
2. Smyth ET, McIlvenny G, Enstone JE, Emmerson AM, Humphreys H, Fitzpatrick F, Davies E, Newcombe RG, Spencer RC; Hospital Infection Society Prevalence Survey Steering Group. Four country healthcare associated infection prevalence survey 2006: overview of the results. J Hosp Infect. 2008 Jul;69(3):230-48. doi: 10.1016/j.jhin.2008.04.020. Epub 2008 Jun 11. [PubMed]
3. Saint S. Clinical and economic consequences of nosocomial catheter-related bacteriuria. Am J Infect Control. 2000 Feb;28(1):68-75. [PubMed]
4. Sheffield JS, Cunningham FG. Urinary tract infection in women. Obstet Gynecol. 2005 Nov;106(5 Pt 1):1085-92. [PubMed]
5. Wazait HD, Patel HR, Veer V, Kelsey M, Van Der Meulen JH, Miller RA, Emberton M. Catheter-associated urinary tract infections: prevalence of uropathogens and pattern of antimicrobial resistance in a UK hospital (1996-2001). BJU Int. 2003 Jun;91(9):806-9. [PubMed]
6. Kucheria R, Dasgupta P, Sacks SH, Khan MS, Sheerin NS. Urinary tract infections: new insights into a common problem. Postgrad Med J. 2005 Feb;81(952):83-6.
7. Dodd MJ, Miaskowski C, Lee KA. Occurrence of symptom clusters. J Natl Cancer Inst Monogr. 2004;(32):76-8. [PubMed]
8. Shapiro M, Simchen E, Izraeli S, Sacks TG. A multivariate analysis of risk factors for acquiring bacteriuria in patients with indwelling urinary catheters for longer than 24 hours. Infect Control. 1984 Nov;5(11):525-32. [PubMed]
9. Wald HL, Ma A, Bratzler DW, Kramer AM. Indwelling urinary catheter use in the postoperative period: analysis of the national surgical infection prevention project data. Arch Surg. 2008 Jun;143(6):551-7. doi: 10.1001/archsurg.143.6.551.
10. Plowman R, Graves N, Esquivel J, Roberts JA. An economic model to assess the cost and benefits of the routine use of silver alloy coated urinary catheters to reduce the risk of urinary tract infections in catheterized patients. J Hosp Infect. 2001 May;48(1):33-42.
11. Garibaldi RA, Burke JP, Dickman ML, Smith CB. Factors predisposing to bacteriuria during indwelling urethral catheterization. N Engl J Med. 1974 Aug 1;291(5):215-9. [PubMed]
12. Schaeffer AJ. Catheter associated bacteriuria. The Urologic Clinics of North America 1986; 13(4): 735–47.
13. Sondi I, Salopek-SondiB.Silver nanoparticles as antimicrobial agent: a case study on E. coli as a model for Gram-negative bacteria. J Colloid Interface Sci. 2004 Jul 1;275(1):177-82. [PubMed]
14. Davenport K, Keeley FX. Evidence for the use of silver-alloy-coated urethral catheters. J Hosp Infect. 2005 Aug;60(4):298-303. [PubMed]
15. Crosby-Nwaobi RR, Faithfull S. High risk of urinary tract infections in post-operative gynaecology patients: a retrospective case analysis. Eur J Cancer Care (Engl). 2011 Nov;20(6):825-31. doi: 10.1111/j.1365-2354.2011.01283.x.Epub 2011 Aug 24.
Copyright (c) 2018 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative





