Comparative study between pull (reverse breech technique) and push (conventional technique) during cesarean delivery in obstructed labor
Abstract
Aims and Objectives: To compare the maternal and neonatal morbidities and to identify the etiology of obstructed labor and retrospective analyze the pull and push techniques for delivery of impacted head during cesarean section.
Method: This observational study was conducted in IPGME and R, SSKM medical college from April 2015 to Feb 2019. The study population included 74 women tackled with the pull method, while the control group comprised 74, age and parity matched who underwent the push method of head delivery.
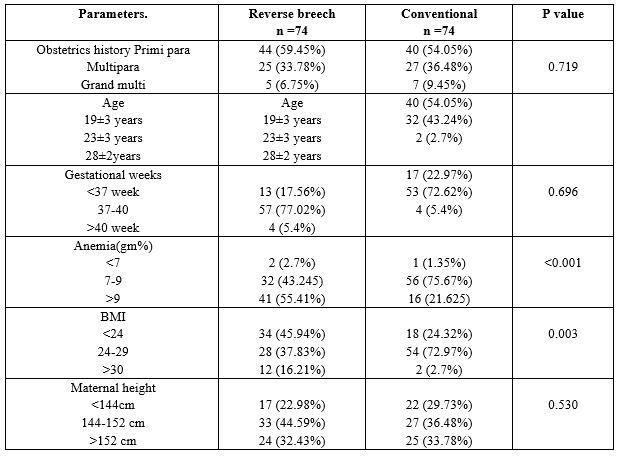
Results: A review of 74 patients revealed the average age of the study population was 25.7±2 years. Patients with anemia (Hb≤8.5 to 10gm/dl) and abnormal BMI (>30and<24) were observed to suffer more from obstructed labor (p≤0.050). On the other hand, maternal height was not found to predict obstructed labor(p=0.5300). Patients with pull methods were noted to have less intra-operative fetal complication i.e. uterine artery injury (4 VS 19; P≤0.O5) transverse excision of the uterine incision (8vs 19; p≤0.05), vertical extension (1 vs 14; p ? 0.05)). Post-operative morbidity was also less, like fever( 01 vs31 ;p≤ 0.05), wound infection (2 vs 12; p≤ 0.05) and blood transfusion requirement (7 vs 16; p≤ 0.05), hospital stay more than seven days (4 vs 22; p≤ 0.05), There was no significant statistical difference between either group in terms of neonatal outcome.
Conclusion: Although the pull method may lead to some neonatal complications, it is associated with lower maternal morbidity than push method in impacted fetal head extraction during cesarean delivery. Thus, this method of head delivery may enable a better fetomaternal outcome in obstructed labor.
Downloads
References
Ould El Joud D, Bouvier-Colle M-H, MOMA Group. Dystocia: study of its frequency and risk factors in seven cities in west Africa. Int J Gynaecol Obstet. 2001;74(2):171-178. doi: https://doi.org/10.1016/s0020-7292(01)00407-6.
Dolea C, Abu Z, Global burden of obstructed labor in the year 2000, Global burden of Disease 2000 Evidence andInformation for policy (EIP), WHO, Geneva,2003. doi: https://www.who.int/healthinfo/statistics/bod_obstructedlabour.pdf.
Maternal Mortality Update-UNFPA Assistance of Maternal Mortality Prevention Activities: An Overview.1998-1999. Available at https://www.unfpa.org/sites/default/files/pub-pdf/Maternal_Death_Surveillance_and_Response_0.pdf.
Murray, Christopher J. L, Lopez, Alan D and World Health Organization. (1998). Health dimensions of sex and reproduction : the global burden of sexually transmitted diseases, HIV, maternal conditions, perinatal disorders, and congenital anomalies / edited by Christopher J. L. Murray, Alan D. Lopez. Boston: Harvard School of Public Health. https://apps.who.int/iris/handle/10665/42161.
Fortney JA, Smith JB. Measuring maternal morbidity, in Safe Motherhood Initiatives:critical issues. Eds. Berer M and Ravindran TKS. Reproductive Health Matters, Blackwell Science, 1999.
Fasubaa OB, Ezechi OC, Orji EO, Ogunniye SO, Akindele ST, Loto OM, et al, Delivery of the impacted head of the fetus at cesarean section after prolong obstructed labor: a randomized comparative study of two methods. J Obstet Gynaecol. 2002;22(4):375-378. doi: https://doi.org/10.1080/01443610220141290.
Levy R, Chernomoretez T, Appleman Z, Levin D, Or Y, Hagay ZJ. Head pushing versus reverse breech extraction in cases of impacted fetal head during cesarean section. Eur J Obstet Gynec Reprod Biol 2005; 121(1):24-26. doi: https://doi.org/10.1016/j.ejogrb.2004.09.014.
Mukhopadhay P, Naskar T, Dalui R, Hazra S, Bhattacharya D. Evaluation of patwardhan’s technique –a four year study in a rural teaching hospital. J Obstet Gynecol India. 2005;55:244-246.
Mason L, Glenn S, Walton I, Appleton C. The prevalence of stress incontinence during pregnancy and following delivery. Midwifery, 1999,15(2):120-128. doi: https://doi.org/10.1016/s0266-6138(99)90008-6.
Viktrup L, Lose MD, Rolff M, Barfoed K. The symptoms of stress incontinence caused by pregnancy or delivery in primiparas. Obstet Gynecol J. 1992;79(6):945-949.
Meyer S, Schreyer A, De Grandi P, Hohlfeld P. The effects of birth on urinary continence: mechanisms and other pelvic floor characteristics. Obstet Gynaecol. 1998;92(4):613-618. doi: https://doi.org/10.1016/s0029-7844(98)00248-8.
Van Kessel K, Reed S, Newton K, Meier A, Lentz G. The second stage of labor and stress urinary incontinence. Am J Obstet Gynecol, 2001;184(7):1571-1575. doi: https://doi.org/10.1067/mob.2001.114856.
Wilson PD, Herbison RM, Herbison GP. Obstetric practice and the prevalence of urinary incontinence three months after delivery. Br J Obstet Gynaecol. 1996;103(2):154-161. doi: https://doi.org/10.1111/j.1471-0528.1996.tb09668.x.
MacArthur C, Lewis M, Bick D. Stress incontinence after childbirth. Br J Midwifery, 1993;1(5):207-213.
Groutz A, Gordon D, Keidar R, Lessing JB, Wolman I, David MP, et al. Stress urinary incontinence: prevalence among nulliparous compared with primiparous and grand multiparous premenopausal women. Neurourol Urodynam. 1999;18(5):419-425. doi: https://doi.org/10.1002/(sici)1520-6777(1999)18:5%3C419::aid-nau2%3E3.0.co;2-z.
Mathers CD, Stein C, Tomijima N, Ma Fat D, Rao C, Inoue M, Lopez AD, Murray CJL.(2002). Global Burden of Disease 2000: Version 2 methods and results. Geneva, Worl Health Organization. Available at https://www.who.int/healthinfo/paper50.pdf.
Dolea C, AbuZahr C Global burden of obstructed labor in the year 2000. Global burden of Disease 2000 evidence and Information for policy (EIP), WHO Geneva, 2003. Available at https://www.who.int/healthinfo/statistics/bod_obstructedlabour.pdf.
Jeve YB, Navti OB, Konje JC. Comparison of techniques used to deliver a deeply impacted fetal head at full dilation: a systematic review and meta-analysis. BJOG. 2016;123;(3):337-345. doi: https://doi.org/10.1111/1471-0528.13593.
Unterscheider J, McMenamin M, Cullinane F. Rising rates of caesarean deliveries at full cervical dilatation: concerning trend. Eur J Obstet Gynaecol Reprod Biol. 2011;157(2):141-144. doi: https://doi.org/10.1016/j.ejogrb.2011.03.008.
Veisi F, Zangeneh M, Malekkhosravi S, Rezavand N. Comparison of "push" and "pull" methods for impacted fetal head extraction during cesarean delivery. Int J Gynaecol Obstet. 2012;118(1):4-6. doi: https://doi.org/10.1016/j.ijgo.2011.12.027.
Saha PK, Gulati R, Goel P, Tandon R, Huria A. Second stage caesarean section: evaluation of patwardhan technique. J Clin Diagn Res. 2014;8(1):93-95. doi: https://doi.org/10.7860/jcdr/2014/6709.3782.
Berhan Y, Berhan A. A meta-analysis of reverse breech extraction to deliver a deeply impacted head during cesarean delivery. Int J Gynaecol Obstet. 2014;124(2):99-105. doi: https://doi.org/10.1016/j.ijgo.2013.08.014.
Frass KA, Al Eryani A, Al-Harazi AH. Reverse breech extraction versus head pushing in caesarean section for obstructed labour. Saudi Med J. 2011;32(12):1261-1266.
Bastani P, Pourabolghasem S, Abbasalizadeh F, Motvalli L. Comparison of neonatal and maternal outcomes associated with head-pushing and head-pulling methods for impacted fetal head extraction during cesarean delivery. Int J Gynaecol Obstet. 2012;118(1):1-3. doi: https://doi.org/10.1016/j.ijgo.2012.03.005.
Lawson JB.obstructedlabor.In; Lawson JB, Stewart DD, eds Obstetrics and Gynecology in the tropics and developing countries. London; Edward Arnold PRESS, 1967; 172-202.
Konje JC, Lapipo O. Nutrition and obstructed labor. Am J Clin Nutr. 2000;72(1);291S-297S. doi: https://doi.org/10.1093/ajcn/72.1.291s.
Zhang J,Kendric A, Quenby s, wray s Contractility and Calcium Signaling of Human Myometrium are profoundly Affected by Cholesterol Manipulation; Impaction in Labor? Reprod Sci. 2007;14(5):456-466. doi: https://doi.org/10.1177/1933719107306229.
Copyright (c) 2020 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative





