A rare case of prolapse of ovarian cyst through vaginal vault
Rao KG.1*, Rao G.2, Lakshminarayana K.3, Devi K.4
DOI: https://doi.org/10.17511/joog.2020.i01.05
1*K Gangadhara Rao, Professor, Department of Gynaecology, NRI Medical College and General Hospital, Guntur, Andhra Pradesh, India.
2 G Srinivasa Rao, Professor, Department of Urology, NRI Medical College and General Hospital, Guntur, Andhra Pradesh, India.
3 Lakshminarayana K, Professor, Department of Family Medicine, NRI Medical College and General Hospital, Guntur, Andhra Pradesh, India.
4 K Prabha Devi, Professor, Department of Gynaecology, NRI Medical College and General Hospital, Guntur, Andhra Pradesh, India.
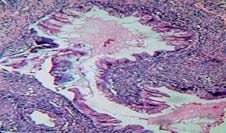
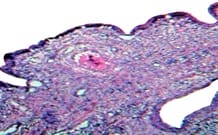
Hysterectomy is the most common gynecological major surgery. It is performed for both benign and malignant conditions of the female genital tract. Common indications of hysterectomy include abnormal uterine bleeding (fibroids, adenomyosis), pelvic inflammatory disease. It can be performed via abdominal or vaginal routes depending on the pathology. In this era of minimally invasive surgery, laparoscopic hysterectomy is gaining popularity. Complications of this surgery depend on the etiology, route of hysterectomy and the technique used. Common complications of this procedure include infections, hemorrhage, thromboembolism, urinary tract, gastrointestinal injury. Vault prolapse can also occur years after performing a hysterectomy. Prolapse of fallopian tubes and omentum through the vault have been reported. However, prolapse of other abdominal and pelvic organs like bowel, ovary, and bladder through the vaginal vault is a rare entity. Prolapse of the ovarian cyst through vaginal vault has so far not been reported in the world literature. The present case report was of a very rare case of ovarian cyst prolapse through the vaginal vault in a 35-year-old woman; which was successfully treated by laparotomy and ovarian cystectomy. Her post-operative histopathology was suggestive of mucinous cystadenoma. Her post-operative period was uneventful, and she was discharged in a stable condition.
Keywords: Ovarian cyst - Prolapse, Vault, Post Hysterectomy
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor, Department of Gynaecology, NRI Medical College and General Hospital, Guntur, Andhra Pradesh, India. Email:  |
Rao KG, Rao GS, Lakshminarayana K, Devi KP. A rare case of prolapse of ovarian cyst through vaginal vault. Obs Gyne Review J Obstet Gynecol. 2020;6(1):28-31. Available From https://obstetrics.medresearch.in/index.php/joog/article/view/99 |
 |
 ©
©