Study Of Fetomaternal Outcome In Cases Of Placenta Previa At Tertiary Care Hospital, Dhaka, Bangladesh
Kulsum U1*, Akhtar N2, Parveen T3, Qumruzzaman K4, Wahid F5, Islam N6, Begum Z7, Kulsum SU8
DOI:10.17511/joog.2024.i01.05
1* Umme Kulsum, Assistant Professor, Dept of Fetomaternal Medicine, Bangabandhu Sheikh Mujib Medical College, Dhaka, Bangladesh.
2 Nahreen Akhtar, Professor, Dept Of Fetomaternal Medicine, Bangabandhu Sheikh Mujib Medical College, Dhaka, Bangladesh.
3 Tabassum Parveen, Professor, Dept Of Fetomaternal Medicine, Bangabandhu Sheikh Mujib Medical College, Dhaka, Bangladesh.
4 Khondoker Qumruzzaman, Assistant Professor, Department of Cardiology, Bangabandhu Sheikh Mujib Medical College, Dhaka, Bangladesh.
5 Fatima Wahid, Assistant Professor, Dept Of Fetomaternal Medicine, Bangabandhu Sheikh Mujib Medical College, Dhaka, Bangladesh.
6 Nilufar Islam, Assistant Professor, Dept Of Fetomaternal Medicine, Bangabandhu Sheikh Mujib Medical College, Dhaka, Bangladesh.
7 Zakia Begum, Assistant Professor, Obs and Gynae, Bangabandhu Sheikh Mujib Medical College, Faridpur, Bangladesh.
8 Syeda Ummay Kulsum, Assistant Professor, General Obs and Gynae, Bangabandhu Sheikh Mujib Medical College, Dhaka, Bangladesh.
Background: Placenta previa remains a significant obstetric challenge associated with substantial maternal and fetal morbidity. The increasing incidence of placenta previa and its associated complications, particularly in the context of rising cesarean section rates, necessitates ongoing evaluation of management strategies and outcomes.
Objective: To assess the fetomaternal outcomes in cases of placenta previa managed at a tertiary care hospital and to identify risk factors associated with adverse outcomes.
Methods: This retrospective observational study analyzed 60 cases of placenta previa managed at FetomaternalMedicine Dept., BSMMU, Dhaka, Bangladesh between June 2023 to June 2024. Data on maternal characteristics, obstetric factors, management strategies, and fetomaternal outcomes were collected from medical records. Statistical analysis included descriptive statistics and multivariate logistic regression to identify risk factors for adverse outcomes.
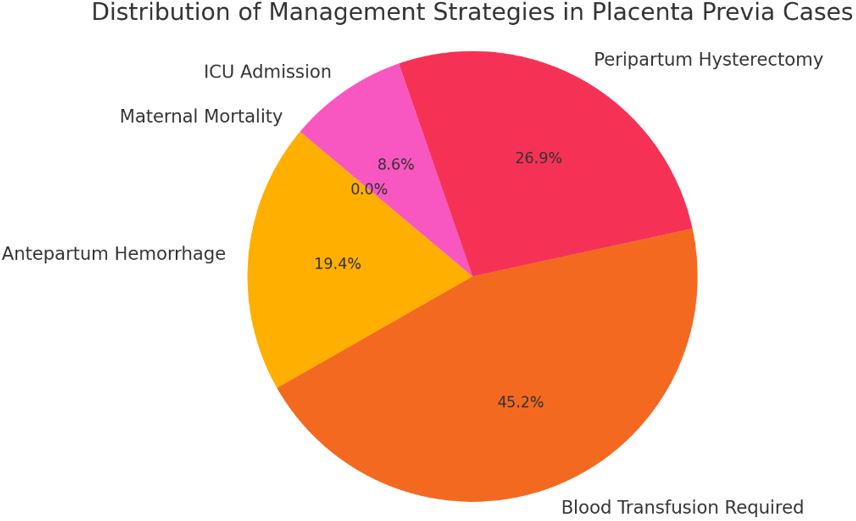
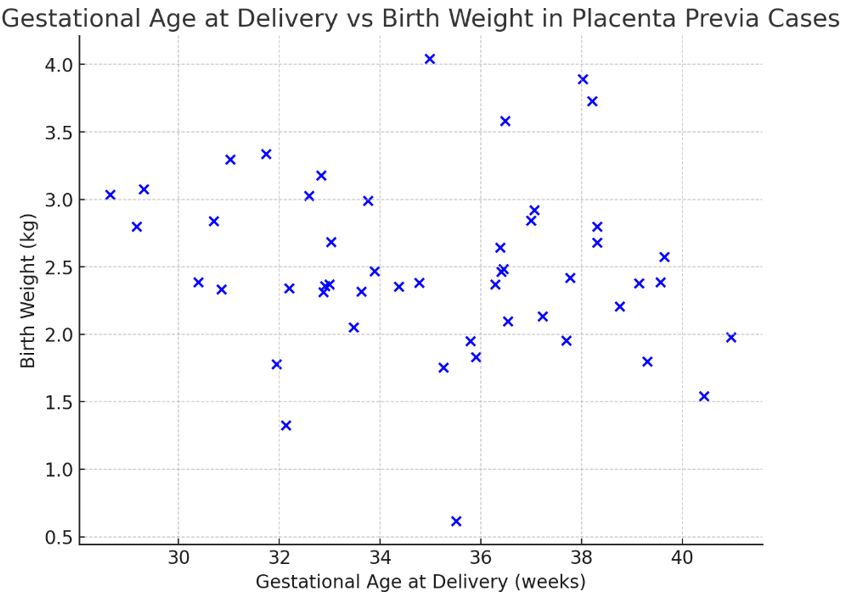
Results: The mean maternal age was 29.2 ± 4.3 years, with 75% of patients having a history of previous cesarean sections. Placenta previa was diagnosed in 76.7% of cases, and low-lying placenta was present in 23.3%. Peripartum hysterectomy was performed in 41.7% of cases. The preterm delivery rate was 70%, with a mean gestational age at delivery of 35.6 ± 2.8 weeks. Neonatal intensive care unit admission was required for 36.7% of newborns, and the perinatal mortality rate was 3.3%. Multivariate analysis identified previous cesarean sections (≥2) (adjusted OR 3.8, 95% CI 1.7-8.5) and placenta accreta spectrum disorders (adjusted OR 12.5, 95% CI 4.2-37.1) as significant risk factors for peripartum hysterectomy.
Conclusion: This study highlights the significant maternal and fetal morbidity associated with placenta previa, particularly in cases with previous cesarean sections and placenta accreta spectrum disorders. The findings underscore the importance of early diagnosis, multidisciplinary management, and the need for specialized care in tertiary centres for high-risk pregnancies. Strategies to reduce primary cesarean section rates and careful counselling for women with a history of cesarean delivery are crucial in addressing this growing obstetric challenge.
Keywords: Placenta previa, placenta accreta spectrum, cesarean section, peripartum hysterectomy, fetomaternal outcome
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Dept of Fetomaternal Medicine, Bangabandhu Sheikh Mujib Medical College, Dhaka, , Bangladesh. Email:  |
Kulsum U, Akhtar N, Parveen T, Qumruzzaman K, Wahid F, Islam N, Begum Z, Kulsum SU, Study Of Fetomaternal Outcome In Cases Of Placenta Previa At Tertiary Care Hospital, Dhaka, Bangladesh. Obs Gyne Review J Obstet Gynecol. 2024;10(1):32-39. Available From https://obstetrics.medresearch.in/index.php/joog/article/view/171 |
 |
 ©
©