Struma Ovarii – A Case Report
Gayam S.1*, Rani G.2, Laxmi VVS3, Trilok.4
DOI: https://doi.org/10.17511/joog.2023.i01.01
1* Susheela Gayam, DNB, DGO– HOD & Senior Consultant, Department of Obstetrics and Gynaecology, Vijay Marie Hospital, Hyderabad, Telangana, India.
2 Geeta Rani, DNB – Senior Consultant, Department of Obstetrics and Gynaecology, Vijay Marie Hospital, Hyderabad, Telangana, India.
3 Laxmi VVS, MS, FRCS, DGO – Laparoscopic Surgeon, Department of Obstetrics and Gynaecology, Vijay Marie Hospital, Hyderabad, Telangana, India.
4 Trilok, MD-Pathologist, Department of Obstetrics and Gynaecology, Vijay Marie Hospital, Hyderabad, Telangana, India.
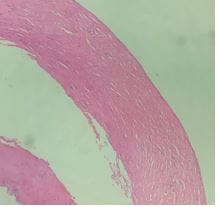
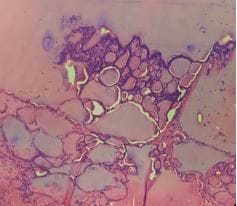
Struma Ovarii is an uncommon variant of ovarian monodermal mature cystic teratoma consisting of thyroid tissue. Preoperative diagnosis of it is difficult as the clinical presentation and ultrasound imaging are often similar to that of ovarian neoplasm. These patients, mostly with benign diseases, often have more extensive surgery than necessary. We present a case report of a 60-year-old patient with a preoperative diagnosis of ovarian neoplasm post-operatively diagnosed as struma ovarii on histopathology which is confirmatory. This case report aims to highlight the importance of associating preoperatively clinical findings and investigations to avoid extensive surgery. When suspected it is crucial to evaluate thyroid status to avoid complications of hyperthyroidism.
Keywords: Monodermal Teratoma, Struma Ovarii, Suspected Ovarian Malignancy, Thyroid Follicles
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , DNB, DGO– HOD & Senior Consultant, Department of Obstetrics and Gynaecology, Vijay Marie Hospital, Hyderabad, Telangana, India. Email:  |
Susheela Gayam, Geeta Rani, Laxmi VVS, Trilok, Struma Ovarii – A Case Report. Obs Gyne Review J Obstet Gynecol. 2023;9(1):1-4. Available From https://obstetrics.medresearch.in/index.php/joog/article/view/159 |
 |
 ©
©