Ovarian Ectopic Pregnancy: Laparoscopic Excision and Ovarian Conservation – Case Report
Gayam S.1*, Rani G.2
DOI: https://doi.org/10.17511/joog.2023.i01.02
1* Susheela Gayam, Consultant, Department of Obstetrics and Gynaecology, Vijay Marie Hospital, Hyderabad, Telangana, India.
2 Geeta Rani, Consultant, Department of Obstetrics and Gynaecology, Vijay Marie Hospital, Hyderabad, Telangana, India.
Ovarian pregnancy is a rare type of non-tubal ectopic pregnancy. 27-year-old primigravida presented with 2 months of amenorrhea with right ectopic pregnancy on routine ultrasonography. But then intraoperatively it was found to be ruptured right ovarian ectopic pregnancy. The similar symptomatology of tubal ectopic pregnancy makes preoperative diagnosis of ovarian ectopic pregnacy difficult. Laparoscopy is the standard management method for haemodynamically stable patients with ovarian ectopic pregnancy. Resection of the ovarian ectopic pregnancy and preservation of the ovary is the mainstay of management in ovarian ectopic pregnancies.
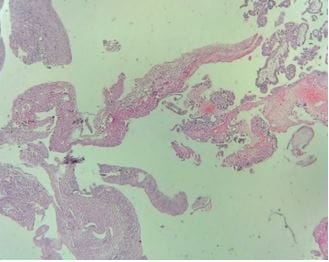
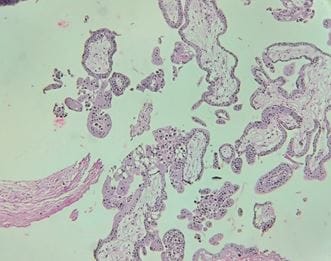
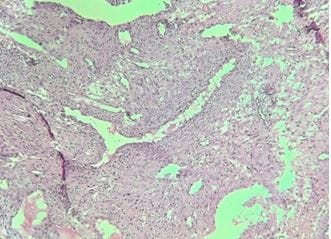
Keywords: Ovarian Pregnancy, Laparoscopic Excision, Ovarian Conservation, Histopathology
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Consultant, Department of Obstetrics and Gynaecology, Vijay Marie Hospital, Hyderabad, Telangana, India. Email:  |
Susheela Gayam, Geeta Rani, Ovarian Ectopic Pregnancy: Laparoscopic Excision and Ovarian Conservation – Case Report. Obs Gyne Review J Obstet Gynecol. 2023;9(1):5-8. Available From https://obstetrics.medresearch.in/index.php/joog/article/view/158 |
 |
 ©
©