Immediate Postpartum Intrauterine Device Insertion and its outcome: a Prospective Study in a Tertiary Care Centre
Pentela G.1*, M Laddad M.2, S Kshirsagar N.3
DOI: https://doi.org/10.17511/joog.2022.i02.03
1* Greeshma Pentela, Postgraduate Resident, Department of Obstetrics and Gynaecology, Krishna Institute of Medical Sciences, Karad, Maharashtra, India.
2 Manisha M Laddad, Associate Professor, Department of Obstetrics and Gynaecology, Krishna Institute of Medical Sciences, Karad, Maharashtra, India.
3 N S Kshirsagar, Professor, Department of Obstetrics and Gynaecology, Krishna Institute of Medical Sciences, Karad, Maharashtra, India.
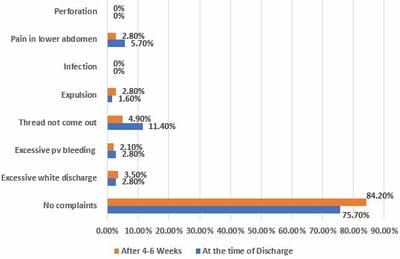
Background: In developing countries, the maternal mortality and morbidity associated with closely related pregnancies and abortions can be prevented by intervening immediately after delivery by providing women with insertion of IUCD. This study was intended to evaluate PPIUCD as a method of contraception immediately following the delivery. Aims and Objectives: To evaluate the acceptability of PPIUCD, various factors affecting its influence, and to study the follow-up complications. Materials and Methods: This study was conducted in the labour room at KIMS, Karad from January 2020 to May 2021. Women around 18-40 years, of 34-40weeks, were included. Pregnancies complicated with PROM>18 hours, obstructed labour, fever, anaemia, and PPH were excluded. After proper counselling, women were inserted with IUCD after 10min-48 hrs of delivery of placenta in vaginal or caesarean section and followed up at discharge and 6weeks. Results: Out of 8128 deliveries, 3534(43.6%) women had fulfilled medical eligibility criteria, out of which 140(40%) women had accepted the service among the counselled women of 350(9.90%). During follow up, 75.7% had no complaints at discharge and 84.2% at 6weeks. Few had excessive bleeding, pain in the lower abdomen, and no visible thread complaints. The overall expulsion rate at 6 weeks in this study was around 2.1% and the continuation rate was 97.8%. Conclusion: There is a need for proper counselling for PPIUCD and conduct workshops from the early weeks of pregnancy to cover the unmet needs of contraception.
Keywords:
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Postgraduate Resident, Department of Obstetrics and Gynaecology, Krishna Institute of Medical Sciences, Karad, Maharashtra, India. Email:  |
Greeshma Pentela, Manisha M Laddad, N S Kshirsagar, Immediate Postpartum Intrauterine Device Insertion and its outcome: a Prospective Study in a Tertiary Care Centre. Obs Gyne Review J Obstet Gynecol. 2022;8(2):19-25. Available From https://obstetrics.medresearch.in/index.php/joog/article/view/155 |
 |
 ©
©