Rate and Indication of Elective Caesarean Section: A Retrospective Study
Shwetha N.1, Harish K.2*, Sai Chandhan T.3, Sreenivasa Reddy C.4, Satish Reddy G.5, Pujith Kumar G.6
DOI: https://doi.org/10.17511/joog.2021.i05.02
1 N Shwetha, Associate Professor, Dept of OBG, Sri Lakshminarayana Institute of Medical Sciences, Pondicherry, Union Territory, India.
2* KM Harish, Associate Professor, Dept of OBG, Apollo Institute of Medical Sciences and Research, Chittoor, Andhra Pradesh, India.
3 T Sai Chandhan, Housesurgeon, Dept of OBG, Apollo Institute of Medical Sciences and Research, Chittoor, Andhra Pradesh, India.
4 C Sreenivasa Reddy, Housesurgeon, Dept of OBG, Apollo Institute of Medical Sciences and Research, Chittoor, Andhra Pradesh, India.
5 GM Satish Reddy, Housesurgeon, Dept of OBG, Apollo Institute of Medical Sciences and Research, Chittoor, Andhra Pradesh, India.
6 G Pujith Kumar, Housesurgeon, Dept of OBG, Apollo Institute of Medical Sciences and Research, Chittoor, Andhra Pradesh, India.
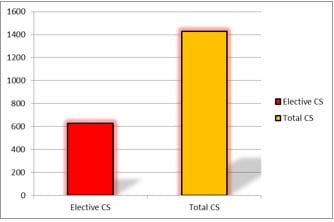
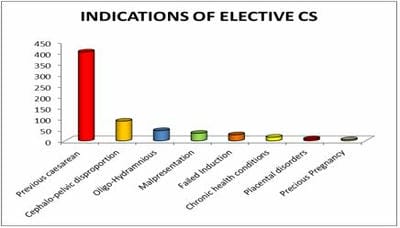
Background: The elective caesarean rate also contributes to increased total caesarean section rates in recent times. This study was undertaken to know the elective caesarean section rate in a district hospital and the indications contributing to it. Method: Sociodemographic data for the elective caesarean section deliveries and indications of elective caesarean sections performed during one year from January 2020 to December 2020 at The Apollo Medical College and Government district hospital, Chittoor were collected in a retrospective manner. Results: Elective caesarean section rate was 43.85%. Booked multigravida women, 20 to 30 years old, studied up to metric, residing in a rural area, belong to middle socioeconomic status were the majority to undergo elective C.S. Repeat C.S. made the most significant contribution to the elective C.S. rate followed by Cephalo-pelvic Disproportion. Conclusions: Repeat C.S. and Cephalopelvic disproportion (CPD) are the most common indications of elective caesarean section.
Keywords: Elective caesarean section, Repeat caesarean section, Cephalopelvic disproportion (CPD)
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Dept of OBG, Apollo Institute of Medical Sciences and Research, Chittoor, Andhra Pradesh, India. Email:  |
N Shwetha, KM Harish, T Sai Chandhan, C Sreenivasa Reddy, GM Satish Reddy, G Pujith Kumar, Rate and Indication of Elective Caesarean Section: A Retrospective Study. Obs Gyne Review J Obstet Gynecol. 2021;7(5):50-56. Available From https://obstetrics.medresearch.in/index.php/joog/article/view/146 |
 |
 ©
©