Abnormal Uterine Bleeding- Its Causes and Management in Women with Reproductive Age
Khanam A1*, Bushra A2, Hossain SN3, Akter T4, Zahan N5, Dina US6, Minkin T7
DOI:https://doi.org/10.17511/joog.2024.i01.09
1* Afroja Khanam, Assistant Registrar, Department of Obstetrics and Gynecology, Cumilla Medical College Hospital, Cumilla, Bangladesh.
2 Anika Bushra, Registrar, Department of Obstetrics and Gynecology, BRB Hospital, Dhaka, Bangladesh.
3 Syeda Najiba Hossain, Indoor Medical Officer, Department of Obstetrics and Gynecology, Dhaka Medical College and Hospital, Dhaka, Bangladesh.
4 Tasmia Akter, MBBS, FCPS. MCPS, DGO (Obs and Gynae), Gynaecologist, CMH, Chittagong, Bangladesh.
5 Nusrat Zahan, Medical Officer, Department of Obstetrics and Gynecology, Barkal Upazila Health Complex Rangamati, Chattogram, Bangladesh.
6 Umme Salma Dina, Registrar, Department of Obstetrics and Gynecology, Mymensingh Medical College Hospital, Mymensingh, Bangladesh.
7 Tanmina Minkin, Consultant, Department of Obstetrics and Gynecology, Popular Diagnostic Centre Ltd, Kushtia, Bangladesh.
Introduction: Abnormal uterine bleeding (AUB) is defined as bleeding from the uterine corpus that is abnormal in regularity, volume, frequency or duration and occurs in the absence of pregnancy. It makes the patient uncomfortable and hampers social, familial and religious life.
Methods: A cross-sectional observational study was carried out among 100 women of reproductive age admitted to the Obstetrics and Gynecology department of Comilla Medical College Hospital. The study duration was 6 months, from January 2022 to July 2022. Patients were properly explained about the study and informed consent was taken. Analysis of these women is done by recording age parity, menstrual symptoms and treatment options. All specimens were sent for histopathology. Etiology, clinical presentation, histopathological findings and USG reports were correlated. AUB was classified according to the PALM-COEIN classification.
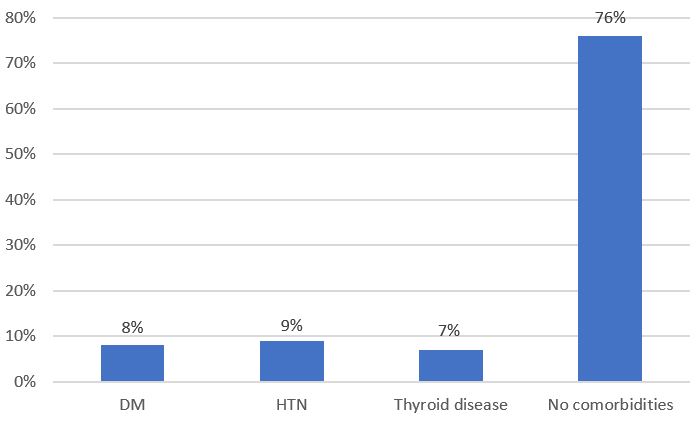
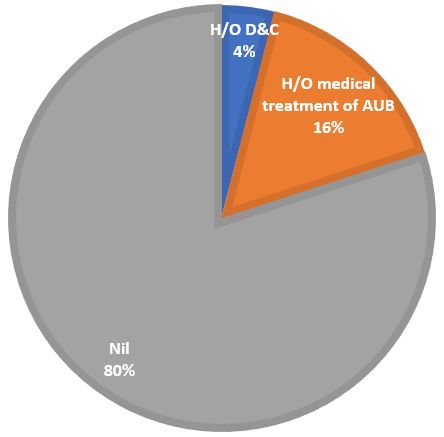
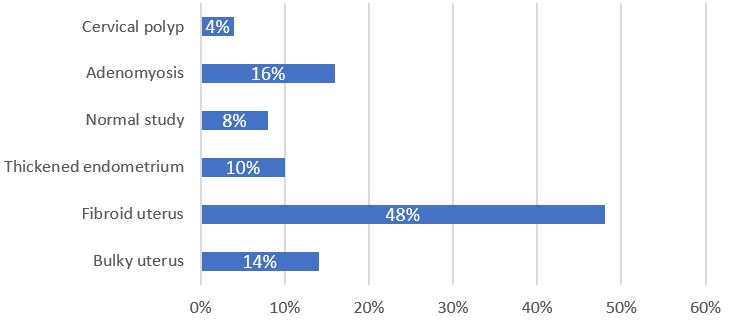
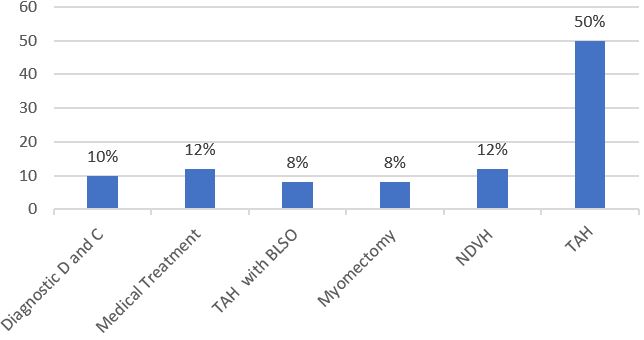
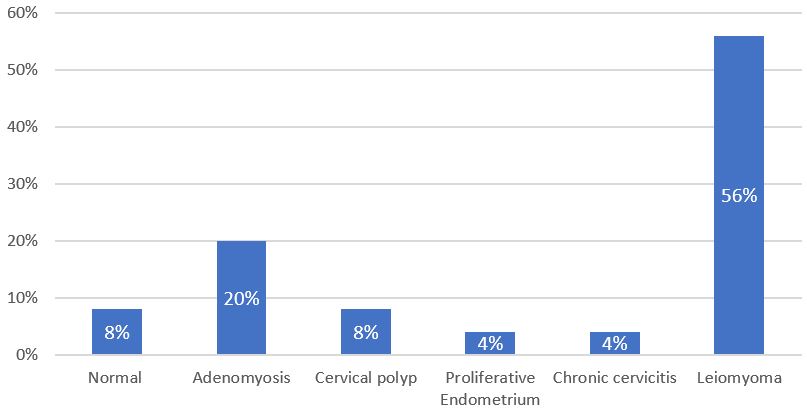
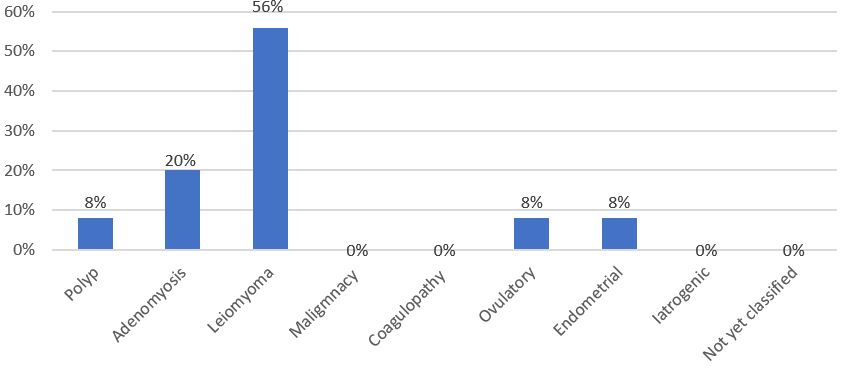
Results: In this study, most of the patients revealed the common age group 31-40 years (50%) and most of them (64%) belonged to average economic conditions. 76% patient were multiparous. Heavy menstrual bleeding was a common presentation (48%).8% of patients were treated medically. Different operations were done among them total abdominal hysterectomy was done in 60% of cases, non-descent vaginal hysterectomy was done in 12% of cases, and diagnostic dilatation and curettage were done in 10% of cases. As per PALM-COEIN classification AUB (L) was a common type and most of the patients belong to the PALM group (84%)
Conclusions: A systematic approach to diagnosis, investigation and a step-wise approach to intervention is necessary. Treatment commencing with medical therapeutic modalities followed by surgical modalities is the ultimate goal of all therapeutic interventions.
Keywords: Abnormal Uterine Bleeding, Prevalence, Causes
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Registrar, Department of Obstetrics and Gynecology, Cumilla Medical College Hospital, Cumilla, , Bangladesh. Email:  |
Khanam A, Bushra A, Hossain SN, Akter T, Zahan N, Dina US, Minkin T, Abnormal Uterine Bleeding- Its Causes and Management in Women with Reproductive Age. Obs Gyne Review J Obstet Gynecol. 2024;10(1):66-72. Available From https://obstetrics.medresearch.in/index.php/joog/article/view/174 |
 |
 ©
©