Twin Reversed Arterial Perfusion Syndrome (TRAP or Acardiac Twin) – A Case Report
Rani G1*, Gayam S2, Tabassum A3, Navyasri4
DOI:https://doi.org/10.17511/joog.2023.i01.01
1* Geeta Rani, Consultant, Department of Obstetrics and Gynaecology, Vijay Marie Hospital, Hyderabad, Telangana, India.
2 Susheela Gayam, Consultant, Department of Obstetrics and Gynaecology, Vijay Marie Hospital, Hyderabad, Telangana, India.
3 Asma Tabassum, Consultant, Department of Obstetrics and Gynaecology, Vijay Marie Hospital, Hyderabad, Telangana, India.
4 Navyasri, Consultant, Department of Obstetrics and Gynaecology, Vijay Marie Hospital, Hyderabad, Telangana, India.
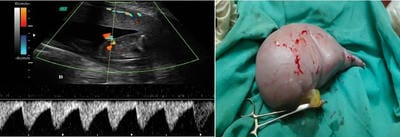
Acardiac Twin known as TRAP (Twin Reversed Arterial Perfusion) syndrome is a rare and serious complication of mono-zygotic multiple gestation. This results in the existence of an Acardiac twin which fails to develop the head, upper limbs, and heart and is dependent upon a normal twin to provide circulation using vascular anastomosis. The pump twin although structurally normal will have high morbidity and mortality. This case report presents an antenatally diagnosed mono-chorionic twin pregnancy with delivery of a normal twin and Acardiac amorphous co-twin.
Keywords: Cardiac Twin, Fetal Anomaly, Twin Reversed Arterial Perfusion Syndrome
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Consultant, Department of Obstetrics and Gynaecology, Vijay Marie Hospital, Hyderabad, Telangana, India. Email:  |
Rani G, Gayam S, Tabassum A, Navyasri, Twin Reversed Arterial Perfusion Syndrome (TRAP or Acardiac Twin) – A Case Report. Obs Gyne Review J Obstet Gynecol. 2023;9(2):9-11. Available From https://obstetrics.medresearch.in/index.php/joog/article/view/163 |
 |
 ©
©